About 2,400 years ago, Hippocrates, the father of medicine, stressed the importance of ethics and objective observation of patients in medicine, breaking away from beliefs in the spells and superstitions trusted until then. However, in each subsequent era, there were still cases of reliance on irrational medical treatments which would be rejected today, but which were conducted due to a lack of scientifically-based knowledge in science and engineering, all while individual physicians maintained a sense of ethics.
It is also said that half of the progress in medicine is owed to the development of science and technology in matters unrelated to medicine. In particular, the application of quantum theory, particle accelerators, and electronics, which blossomed in the 20th century, is often unthinkable in medical schools that do not include these fields in their curriculum. In the present 21st century, where information science and molecular biology have been integrated into medicine, we need professionals with scientific and engineering knowledge who can utilize the most advanced science and technology in medicine; this is in addition to conventional research and researchers working in basic and clinical medicine working to elucidate the physiology of the human body and the pathology of disease, and to help people suffering from illnesses.
To train such professionals conversant with science and technology, Hokkaido University newly established a graduate school, the “Graduate School of Biomedical Science and Engineering” on April 1, 2017. Biomedical science and engineering is a new term, and it is an academic discipline engaged in research to elucidate life phenomena, overcome diseases, and improve human health while utilizing knowledge and technology from science and engineering. In this new graduate school, we aim to undertake a scientific pursuit of the very basics of life, disease, and human health, and to translate the results of our research into developing a medical specialty to help people around the world to live in peace.
Further, as a university facility to conduct international research and to train international scientists of biomedical science and engineering, the Global Center for Biomedical Science and Engineering was established at the Hokkaido University Faculty of Medicine on April 1, 2020. The center is expected to support researchers who pursue medical projects and endeavors using innovative science and engineering with a strong sense of ethics, conducting research and applying cutting-edge technology to medicine, develop new medical technologies and devices, and become able to diagnose and cure the large number of diseases that it has not been possible to treat to date.
We are in this situation today because of the foresight of our predecessors at the dawn of medical science, building on the efforts of researchers who may at times have forgotten to eat and sleep even, to move forward with the accumulated dedicated efforts of supporters, and in the peaceful state of society. However, in Japan, where “action before words” is considered a virtue, it is often difficult to trace the origins of an organization because the history of the organization may have disappeared from the memory of people. With this background, we wish to describe as objectively as we can the events leading up to the establishment of the “Global Center for Biomedical Engineering and Science”.
Please note that the following omits honorifics and titles.
2. Dawn of “Biomedical Science and Engineering Research”
The origin of biomedical science and engineering can be dated to go back to an experiment by Dr. Röntgen, a professor of physics. On November 8, 1895, he reported that he was able to see the bones clearly inside his hand held in front of a fluorescent plate, and that the surrounding soft tissue appeared only weakly, as a faint silhouette when he passed the discharge current from a large induction coil through a vacuum tube (Science 3;227-231, 1896). Since then, researchers of science and engineering developed new disciplines in the 20th century, such as with radioactive materials, the photoelectric effects, particle theory, the theory of relativity, and electronic calculators, which had not been understood by the engineering of the 19th century, and these were then being applied to medicine.
After the second World War, Hokkaido University established a Department of Radiation Medicine in the Faculty of Medicine in 1949, following the establishment of the Research Institute of Applied Electricity in 1946. Masaru Wakabayashi, the first professor here, was from the Research Institute of Applied Electricity via the laboratory of physiology, and Goro Irie, the second professor, enrolled in the School of Medicine of Hokkaido University after graduation from the Faculty of Science. At first, these two researchers were engaged in research in what should be called “biomedical science and engineering” rather than “medical science”. In the 1950s, they engaged in research into the indirect effects of radiation, and in the early 1960s, published many papers of research on solid-state dosimeters that could monitor irradiation sites in three dimensions, and presented the findings at many conferences. In the latter half of the 1960s, they conducted industry-academia collaborative research with Shimadzu Corporation, research which incorporated remote control to prevent surgeons from being exposed to radiation while performing radium treatment for cervical cancer patients (1), and in the 1970s, they created a patient database using a large computer, and worked with a private company (Shimadzu Corporation) on research, and from around 1980 on development of CT systems for radiation therapy planning (2).
From the 1980s, the demand for radiologists in clinical settings in Japan rose sharply, and their daily work shifted to mostly performing diagnostic imaging and radiotherapy in hospitals. Topics of conference presentations were mainly about clinical research, and the number of faculty and student researchers engaged in research related to “biomedical science and engineering” as in the past has decreased dramatically. Opportunities to conduct collaborative research with science and engineering departments also became fewer, experimental tools, such as X-ray equipment, flasks, and gas burners disappeared from the classroom at the west wing end of the first floor of the south wing of the School of Medicine. At last, laboratories and a darkroom for developing images became “doctors’ storerooms”, and disappeared over time. In the radiology department, the use of diagnostic and therapeutic equipment imported from overseas has increased, and industry-university collaborative research by domestic medical equipment development companies decreased. This change increased the opportunities for excellent clinical research.
In the latter half of the 1980s, Irie shifted the focus of his research from radiotherapy to medical informatics. As will be described below, in a company (NEC) collaboration project, Irie developed the Picture Archiving and Communication System (PACS), which enables centralizing the management of medical image information in CT and MRI images throughout the hospital and transmitting the information inside and outside the hospital. In this way, Irie contributed to medicine with the “biomedical science and engineering” that integrate medical informatics and radiologic science (3).
3. Development of “Biomedical Science and Engineering Research”
Since 1980, radiology science has become increasingly complex and the importance of physics knowledge in radiotherapy has increased. In Europe and the United States, medical physicists, researchers with master's and doctoral degrees from science and engineering backgrounds have played an important role as responsible for quality control of radiotherapy in hospitals. The WHO and IAEA have recommended that quality control in radiotherapy is essential. However, in Japan, physicians and qualified radiologists have so far been engaged in these duties. In Japan, there were increasing numbers of people who think it necessary to involve researchers of science and engineering in hospital work for the development of radiological science. However, physicians and technologists had no option but to conduct “medical physics” research by themselves, learning by trial and error. In the late 1980s, in a research team led by Irie, Hirohiko Tsujii, Junetsu Mizoe, Takuro Arimoto, Tadashi Kamada, and Yoshiharu Watanabe, a radiologist, and others improved the accuracy of three-dimensional irradiation by using a CT system for treatment planning, and administered large-doses of oligodendrocytes three-dimensionally for lung cancer using thin X-ray beams, probably as the first time worldwide.
In the early 1990s, Hiroki Shirato improved the “Komai-style” cranial fixation device for stereotactic brain surgery, which enabled performance of surgery on intracranial lesions with an accuracy of ±1mm based in the CT and angiography. Shirato also independently developed a fixation device and calculation software to accurately treat tumors deep inside the brain with X-rays from outside the body. Based on the principles reported in a paper written by researchers at Harvard University, Shirato wrote the basic program for the calculation software in BASIC, and completed it with the help of a physician, Toru Matsuzawa, and others. Watanabe, Katsuhisa Fujita and others improved the linear accelerator operation for stereotactic radiotherapy, and Keishiro Suzuki, Takeshi Nishioka, Kenji Kagei and others engaged in clinical research on intracranial tumors, auditory schwannomas, and cerebral arteriovenous malformations, among other challenges. Later, Mizuho Corporation, which had developed the “Komai-style” ring for stereotactic radiotherapy, became interested in that clinical research, and jointly with Hokkaido University developed a fixing device for head immoblization in stereotactic radiotherapy and the associated calculation software, and marketed it as RADFRAME (4). Hidefumi Aoyama and his colleagues actively conducted multicenter clinical research on metastatic tumors using this device, and published the results in international major medical journals, receiving international acclaim, including mentions in the top 1% for citations of papers (5).
Around 1995 Shinichi Shimizu and his colleagues started research into an irradiation method using CT and MRI image analysis. They aimed to make it possible to accurately irradiate from outside the body in cases where tumors of patients with lung and liver cancers move up down, and left right, due to respiration, and tumors of prostate cancer that change the location slightly due to intestinal gas (6). Shirato et al. conducted basic research in collaboration with Tatsuya Kunieda, from the research laboratory of Mitsubishi Electric Corporation, under a Grant-in-Aid for Scientific Research (B) “real-time tumor-tracking radiotherapy” from 1997 to 1998, aiming to expand the area of accuracy achieved in stereotactic irradiation of the brain to include the torso. Shirado et al. made it possible to recognize the movement of 1-2 mm gold markers routinely recorded on videotape of X-ray fluoroscopy equipment every 0.03 seconds by applying pattern recognition technology using a “real-time motion tracking program”, which was the most advanced science and engineering technology at that time. Shirado et al. proposed the invention of synchronous gating radiotherapy to irradiate gold markers only when they are located within ±1 to 2 mm of the planned 3D coordinates, and obtained an international patent for this (Mitsubishi Electric 50%, Hokkaido University 50%). In 1998, the actual device was developed as the “Real-time Tumor-tracking Radiotherapy System” (7), and many papers were published by Shimizu, Rikiya Onimaru, Kei Kitamura, and others related to this research. For a long time, “data on the movement of gold markers in the body obtained by the real-time tumor-tracking system” had been available only at Hokkaido University. For this reason international researchers from Harvard University, the National Cancer Center of the Netherlands, and other institutions gathered in Sapporo to conduct joint research (8, 9, 10). In the 2000s, the number of citations for papers on irradiation techniques frequently led these to become top 1% among cited papers.
In 1995, Nagara Tamaki from Kyoto University was appointed as professor in the Department of Nuclear Medicine of Hokkaido University, and cyclotron positron emission tomography (PET) was introduced to Hokkaido University Hospital. In 1999, a “Tracer Information Analysis Course”, the first endowed chair in the School of Medicine, was made available to develop nuclear medicine research. There, Tohru Shiga, Yuji Kuge, and Chietsugu Kato were in charge of clinical, pharmaceutical, and measurement systems, respectively, enabling highly quantitative analysis work.
Around 1996, Nishioka started molecular biological research to estimate the effects of radiotherapy for head and neck cancers. Nishioka was appointed professor at the Graduate School of Health Sciences at a young age, and laid the foundations for research integrating molecular biology and radiotherapy receiving Grants-in-Aid for Scientific Research (B) related to radiobiology as a principal investigator four times until 2014.
Now it is time to introduce one of the stories behind all of this. The original raw data of the “movement of gold markers in the body obtained by the real-time tumor-tracking system” were useless as recorded because the data contained artifacts such as the details of technician adjustments of the patient body movements, which is different from the movement in the patient body. Distinguishing this from the valuable data of the movement of the body became possible only after enthusiastic efforts by medical doctors including Shimizu and his colleagues, who “cleaned up the data needed for scientists and engineers to perform the analysis” (14). Similarly, there have been many cases where medical doctors presented results of analysis at conferences, using the data where scientists and engineers removed noise generated by the equipment. The “data cleaning” of all medical information is subcontracted work, and had never attracted attention, but in practice, an environment that allows “medical/biological” and “physical/engineering” scientists to work behind the scenes with mutual respect is the essence of “biomedical science and engineering” research.
4. Interdepartmental Collaboration and Large-Scale Industry-Academia Collaboration
In the early spring of 2004, Professor Yoshiaki Kiyanagi of the Faculty of Engineering met Professor Kazuo Miyasaka of the Department of Radiology at the Faculty of Medicine, and proposed that they should work to establish a particle therapy facility in Hokkaido University. Shirato, who was the head of radiotherapy at the time, took charge of tasks such as the secretariat functions. On Tuesday, June 15, 2004, the first preparatory meeting for the promotion of the Hokkaido Biomedical Innovation Project was held at the expense of the participants. The meeting took place in the conference room of the Department of Radiology, School of Medicine (on the first floor of the South Building at that time), and Miyasaka, Tamaki, and Shirato from the School of Medicine, Sadafumi Sawamura, Takeaki Enoto, Shigeru Tadano, and Kiyanagi from the School of Engineering, and Hiroyuki Date and Kato from the School of Health Sciences attended the meeting. They informally named the project group POLARIS, which comes from the first letters in Particle, Oncology, Light, Atom, Radiation, and Imaging Science, and it was decided to promote research that integrated medicine, engineering, and science, encompassing particle therapy, oncology, light, atoms, radiation, and imaging science. The group name, POLARIS is also the name of the North Star Polaris, expressing the aspiration to make this a “project of Hokkaido University, the star of northern Japan, to serve as a navigation mark to keep researchers striving in the right direction without distraction by the various speculations and trends of the world”. People from Hokkaido Electric Power Company, Hitachi, and Mitsubishi Electric were invited to the monthly meetings of POLARIS, and actively took part in the discussions of the introduction of the particle therapy facility.
In 2005, the endowed chair “Molecular Imaging Course” was established by Hitachi, following the earlier endowed chair “Tracer Information Analysis Course”. The head office of Hokkaido University decided to support a project that integrated the research by the endowed chairs and POLARIS, aiming at “Establishment of a platform for cross-departmental and cross-disciplinary collaboration research to promote advanced medicine that integrates medicine and engineering based on molecular imaging research”.
In 2006, the Division of Molecular Tracking and Radiation Medicine Endowment of Hokkaido University Hospital (donors: Hokkaido Electric Power Company, and others) was established to contribute to the community and to train medical physicists. Masayori Ishikawa, a holder of the degree of medical physics, Ryusuke Suzuki, Naoki Miyamoto, Gerard Berenguer, and Kenneth Sutherland, joined the project and started working as science and engineering PhDs in the endowment donated department at the hospital. Further, when Mitsubishi Electric withdrew from the X-ray therapy field in 2004, the company offered to transfer its 50% of the patent for real-time tumor-tracking radiotherapy technology to Hokkaido University, free of charge, and the intellectual property became a 100% owned patent of Hokkaido University. The Division of Molecular Tracking and Radiation Medicine Endowment of Hokkaido University Hospital kept the real-time tumor-tracking technology inherited from Mitsubishi Electric moving along and made the program available for general use. This later became the most important feature of biomedical science and engineering research at Hokkaido University, and led to large-scale research and development related to the real-time tumor-tracking radiotherapy technology.
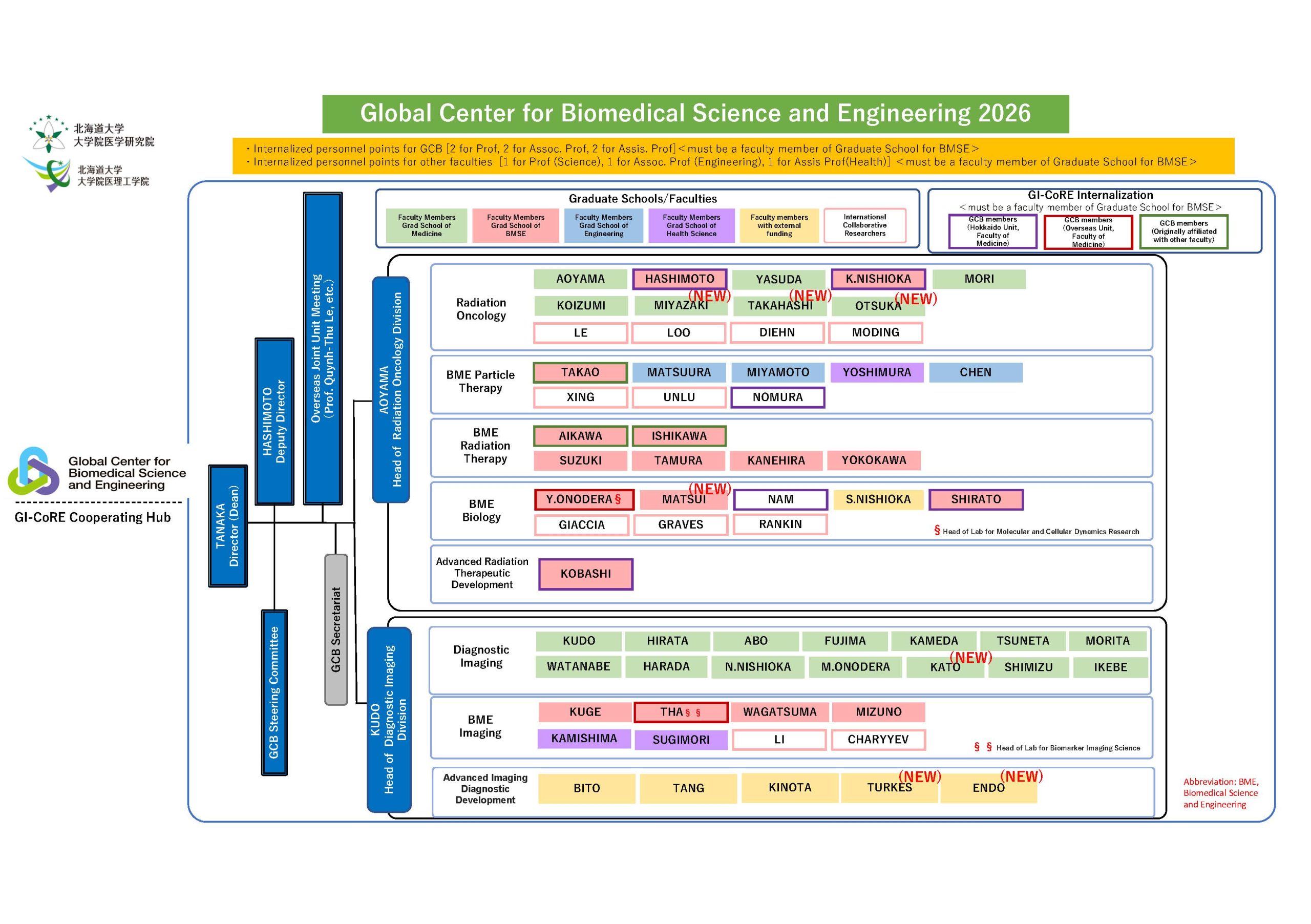
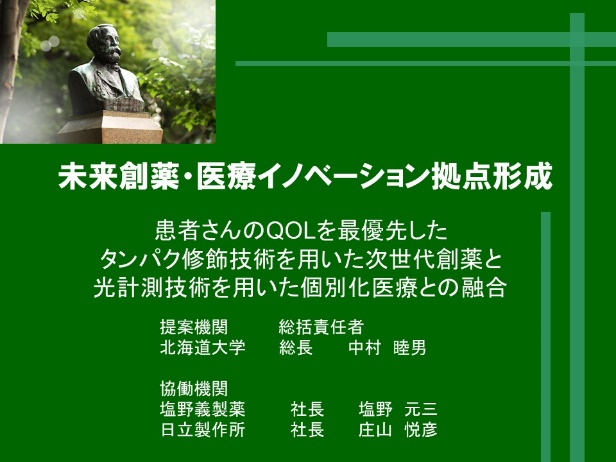
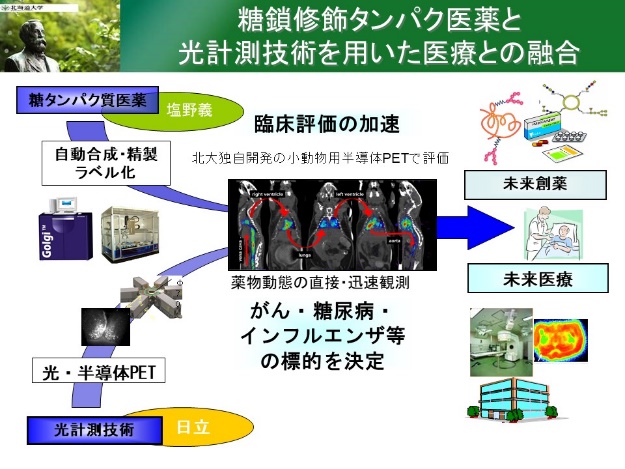
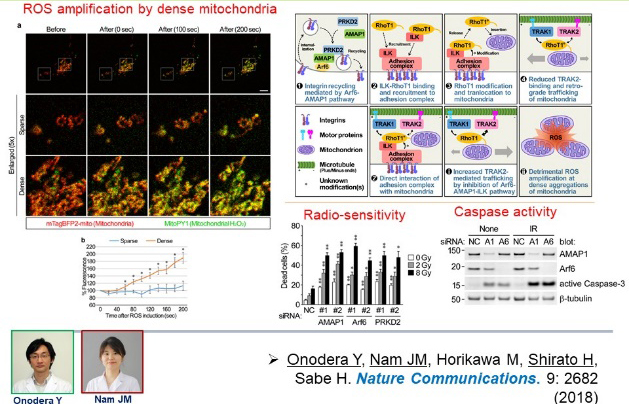
In the same year, 2006, based on the activities described above, Kenichi Homma (the director of the research institute), Tamaki, Shirato, and others collaborated with Yasuyuki Igarashi, Director of the Faculty of Advanced Life Science of Hokkaido University. They won a large industry-university collaborative research project (about 10 billion yen over 10 years) called “the Matching Program for Innovations in Future Drug Discovery and Medical Care at Hokkaido University” (Innovation Program), and conducted biomedical science and engineering research on molecular imaging for 10 years with major companies including Shionogi, Hitachi, and Mitsubishi Heavy Industries. In the project, Kuge, Kato, and Ishikawa from Hokkaido University, and Kikuo Umegaki from Hitachi took an active part in the development of a semiconductor PET system. In addition, Khin Khin Tha conducted research into the analysis of MRI images, Tsuguhide Takeshima conducted research into integration of radiotherapy and immunotherapy, Jin-Min NAM conducted radiation molecular biology, and Yasuhito Onodera conducted molecular biology research with the drug discovery group.
Fig. 1 Materials used in the hearing for the Innovation Program
In 2008, we won large-scale national projects including the Advanced Medical Development Program (Super specialized area) and the NEDO (Principal Investigator Shirato), and also developed a compact X-ray therapy device in collaboration with the venture company Accuthera Inc. and a real time tumor tracking device that can be connected to Varian's X-ray therapy device, SyncTraX, in collaboration with Shimadzu Corporation. During this period, gold markers for implantation in the body and kits for the implantation were developed together with Olympus (disposable gold markers) and Medikit (iGold). With the support of the Hokkaido Organization for Translational Research (HTR) and the Hokkaido University Hospital Clinical Research and Medical Innovation Center, we have brought these products to the pharmaceutical approval stage, and SyncTrax has been adopted at approximately 20 facilities in Japan as of March 15, 2021. CygneX, a compact X-ray therapy device that tracks moving tumors developed by Acucela, has obtained approvals from the Pharmaceuticals and Medical Devices Agency (PMDA) and the Food and Drug Administration (FDA) (although this device is not yet in actual medical use due to the Darwinian Sea (barrier)).
Fig. 2 Materials used in the NEDO hearing for the development of a compact X-ray therapy device
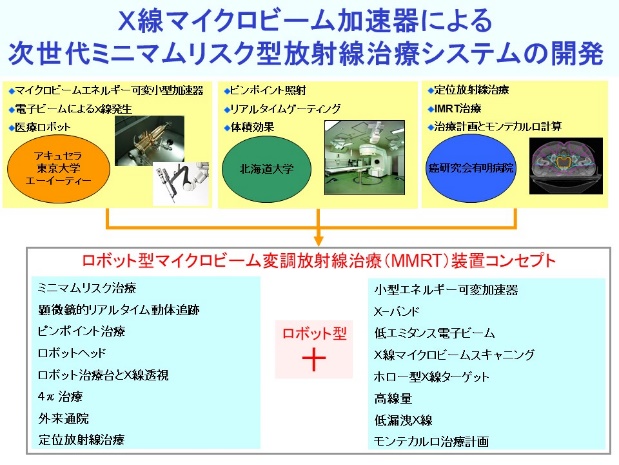
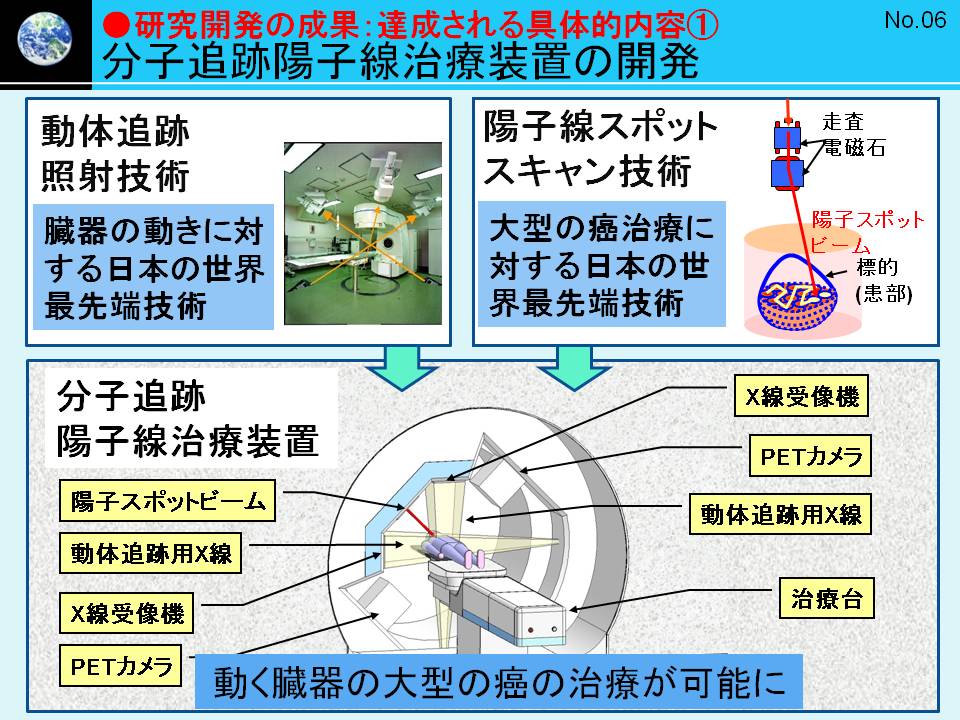
In 2009, we jointly applied for the Funding Program for World-Leading Innovative R&D on Science and Technology (FIRST) with Hitachi and the Graduate Schools of Medicine and Engineering, Hokkaido University. The project involves the “Development of a Real-time Tumor-tracking Radiation Therapy System with Molecular Imaging” incorporating aspects of sustainable development based on research and development that integrates the motion tracking technology and proton beam therapy and it was adopted among the top 30 research projects out of 565 applications (principal investigator Shiroto). With a total cost of approximately 5 billion yen, we developed the PROBERAT-RT, a real-time tumor-tracking proton beam therapy system, and obtained the data necessary for its application as a medical device, contributing to the acquisition of approval for the manufacture of medical devices (11). Hokkaido University built a four-story proton beam therapy center on the premises of Hokkaido University Hospital (approx. 2000m2) at a cost of about 1 billion yen.
Fig. 3 Materials used in the hearing for the Funding Program for World-Leading Innovative R&D on Science and Technology (FIRST)
In this project, as specially-appointed faculty, medical doctors including Shimizu, Takayuki Hashimoto, and Kentaro Nishioka were engaged in the collaborative and translational research till the start of clinical trials. Further, “biomedical science and engineering researchers” including Umegaki, Taeko Matsuura, Chie Toramatsu, Seishin Takao, and Masaya Tamura all at Hokkaido University, produced numerous research achievements in biomedical science and engineering (11-13), and 25 patents related to FIRST (as of December 2013). In 2014, we were invited to the General Council on Science and Technology, and presented our research results in front of Prime Minister Shinzo Abe and Deputy Prime Minister Taro Aso at the Prime Minister’s Office. In 2017, we received the National Commendation for Invention, the Imperial Invention Prize.
In 2013, using the real-time tumor-tracking proton beam therapy system (PROBEAT-RT), the clinical application of POLARIS started at Hokkaido University Hospital, 10 years after the inception of POLARIS. The compact proton therapy device developed in this project has been introduced at a number of the leading hospitals worldwide, such as the Mayo Clinics in Rochester and Arizona, and St. Jude Children's Research Hospital in Spain, Johns Hopkins University Hospital in the U.S.A. Further, PROBERAT-RT is scheduled to be introduced at the M.D. Anderson Hospital in the U.S.A., the National Cancer Center of Singapore (Singapore), and the Hong Kong Hospital for the Aged in China.
Since 2014, the Hokkaido University Hospital Proton Beam Therapy Center has had many visitors (2,225 domestic and 753 from overseas as of January 31, 2020) and trainees (80 domestic and 167 from overseas) who were interested in the worldwide most advanced medical equipment. Among the visitors, there were prominent figures, including Yoshimasa Hayashi, Minister of Education, Culture, Sports, Science and Technology of Japan, and Caroline Kennedy, U.S. Ambassador to Japan. In addition, many medical physicists and other science and engineering faculty from Japanese and overseas institutions came to Hokkaido University Hospital for long-term training.
Since 2017, as a result of intensive work by Shimizu, Matsuura, Miyamoto, Takao, Keiji Kobashi, and their colleagues, we received a large-scale research grant from the Japan Agency for Medical Research and Development (AMED) for the development of a Real-world Adaptive Proton Beam Therapy system based on real-time tumor tracking technology and equipment and systems for quantum radiosurgery, and have promoted industry-university collaborative research on proton therapy with Hitachi.
In 2019, Yuichi Hirata, Shirato et al. proposed the creation of “international standards for radiotherapy” adopted to the movement of tumors in the body by the IEC following an eight-year long development, leading to the publication of the International Electrotechnical Commission IEC TR62926 (15). This led to the publication of IEC TR62926, the International Electrotechnical Commission (15). As a result, the real-time tumor-tracking radiotherapy system developed by Hokkaido University became a standard medical device internationally, not just a device developed by one company.
People often ask us “Why do you need to conduct industry and academia collaborative research, and why do you need to obtain patents?” The reason is that in the case of medical devices, even if a device is developed at a university with the intention of it being useful to patients, the university alone cannot conduct quality control. For this reason, the Pharmaceutical Affairs Law does not allow us to use newly developed medical devices in the clinical setting immediately after the development of such devices. It is always necessary to request a medical device manufacturer with a quality control department to commercialize the product. Another reason for the collaboration with industry is that if universities propose that they hold patents and allow companies to use the patents freely, companies will be more interested in the achievements made by universities. As in Japan we, the universities, did not have such ways of proceeding, we experienced a situation where universities had to purchase expensive imported medical equipment. For this reason, in “Biomedical science and engineering research”, patenting is a “defensive measure” for national universities and the nation, and it is also extremely important for researchers to obtain original data and use the results of the research for the benefit of the world in a scientifically responsible manner.
In the 2010s, the industry-academia collaboration on proton beam therapy expanded greatly. However, as we expect that we will continue to use the equipment itself at Hokkaido University Hospital for 20-30 years, and as of 2021, it will be difficult for the Hospital and medical researchers to develop new equipment for proton beam therapy through large-scale industry-academia collaboration. In this situation, we may have to go back to the original conditions and expect to have to conduct disruptive innovation based on basic research in science and engineering. In the meantime, clinical research on proton beam therapy is steadily progressing in the Department of Radiation Therapy, and we expect the number of clinical studies to increase in the future (16,17). Please keep in mind that the beginning is always the most important, and that it is important to start new research, looking ahead even if it has to be done at the expense of the initiators, like in the case of POLARIS.
5. Biomedical Science and Engineering Research on Digitalization of Medical Information
Irie has made significant achievements as a medical informatics researcher as well as a researcher in radiology. In 1976, he served as the chairman of the Computer System Review Committee of Hokkaido University Hospital, and in 1979, he introduced computers to the hospital as a medical system. He also employed Sachiko Ito, a researcher in science and engineering, as an assistant professor and advanced the research on the digitization of medical information using the large computers at Hokkaido University. He promoted the research and development to computerize medical records and images with SORD, a venture company, and NEC. In 1988, assuming the position as the first director of the Medical Information Department of Hokkaido University Hospital, he launched the PACS, one of the world’s largest imaging information systems at the time jointly developed with NEC, for use in the entire hospital, and its system for placing orders attracting attention from around the world.
After Irie passed away in 1992, Kunihiko Kobayashi, professor of the Laboratory Medicine Division became the second director of the Medical Information Department, followed by Kazuo Miyasaka, professor of radiology, and Tsunetaro Sakurai, professor of medical informatics, Graduate School of Medicine. During this period, due to staff shortages in the Medical Informatics Department, the following staff were employed in working on digitizing all the medical images, medical records, nursing records, and temperature control plates in the Medical Record Management Working Group (WG), Electronic Medical Records WG, Filmless WG: Satoshi Terae, Kosuke Kudo, and Shirato from the Radiology Division; Watanabe, a radiological technologist, from the Radiology Department; and nurses from the Radiotherapy ward. These members of the staff were also engaged in creation of the specifications of the medical information system with Akira Endo from the science and engineering field. In those days, we conducted joint research in the form of discussions on the implementation of the introduced medical information systems without establishing formal joint research agreements. Our numerous ideas were incorporated in the “image information system”, “nursing support system”, “electronic temperature control plate”, and a system that enabled input of information at the bedside using mobile terminals developed by NEC. The image management system, which is connected to the NEC medical information system, and the “Raku Raku Kanjoshisan”, which is a mobile information terminal for use by nurses that displays patient temperatures temporally, are the results of medical science and engineering research conducted by Hokkaido University and NEC.
In April 2004, we developed an “electronic comment” function with Windows Office jointly with NEC, and started to digitize medical record entries in all departments of Hokkaido University Hospital. With this function, we took the first step toward a transition to a completely electronic medical recordkeeping. In May 2004, we succeeded in filmless medical image operation in almost all the departments of the hospital. In this manner we have succeeded the important project to shift to a complete digitalization of medical information. Today the complete digitalization of handling medical information using the medical information systems of NEC became possible because of the efforts of the hospital staff involved in the projects, researchers of the biomedical engineering of NEC, and informatics researchers of science and engineering at Hokkaido University.
For the development of the software, here, if we had concluded a joint research agreement, we would have been able to count the results as achievements of research by Hokkaido University. In the future, the Global Center for Biomedical Engineering and Science is expected to pay attention to concluding agreements for software development in industry-academia collaborations. In 2008, we won a large-scale research grant from NEDO and AMED, and developed a software package called the “Cancer diagnosis and treatment navigation system” jointly with the J-Mac company (Shirato, & Kouichi Yasuda, et al.). This software enables patients to choose among cancer treatments as it fits their perspective. We are currently on the way to commercializing the product and in the process of patenting part of it, but there are still many more matters that could be dealt with through industry-academia collaborative research.
As described above, for the future, we expect to develop software directly related to medical settings through industry-academia collaborative research with medical information-related companies.
6. GI-CoRE GSQ
Since 2010, the increased interest in our research into real-time tumor-tracking proton beam therapy systems with molecular imaging by Europe, the United States, and Asia, we have been awarded a series of public grants related to FIRST. We hold international symposia annually, and become an established research center. This has allowed us to hold the annual international symposiums every year, and attract attention as a research center in this field. At the same time, we face the problem on how to be able to continue long-term collaborative research in areas covering medicine, science, and engineering fields, and also industry-academia collaborative research while training researchers after the end of the FIRST project. Together with the faculty of science and engineering including Umegaki, who had been transferred from Hitachi to become a professor at the Faculty of Engineering, we speculated the options for this and consulted with the university head office.
In 2012, the university head office encouraged us to apply to the World Premier International Research Center Program (WPI) for the “Center for Biodynamics Tracking Medical Science”. We proposed the idea of establishing a center based on real-time tumor tracking technology, molecular imaging, medical materials, and radiation therapy, and received permission to participate from leading researchers at Stanford University as the PI (principal investigator): Professor Lei Xing from the Department of Medical Physics, Professor Amato Giaccia from the Department of Radiobiology, and Professor Quynh-Thu Le from the Department of Radiation Oncology. After a rigorous institutional review, we decided to apply for the WPI as Hokkaido University. However, the Graduate School of Veterinary Medicine of Hokkaido University also applied for the WPI in amphixenosis, and as Hokkaido University did not consolidate the two applications, neither project was adopted.
The following year, the university head office proposed an idea to us, for biomedical science and engineering staff, and the Graduate School of Veterinary Medicine. The proposal is that we should invite researcher units from leading overseas universities to join our unit as part of our efforts to strengthen the functions of the University, and do something about international collaborative research based on the Proton Beam Therapy Center. We consulted with the researchers at Stanford University, who worked together with us in the application to the WPI the year before, and they agreed to cooperate again. We visited Stanford University with Director Kazunori Yasuda, and after repeated discussions with Stanford University, the head office of Hokkaido University, and the Ministry of Education, Culture, Sports, Science and Technology (MEXT), our project to “invite researcher units” was approved, and it was decided to be funded as a special budget item (a time-limited budget in the subsidy for operation) from the following year.
In 2014, using the special funds of MEXT for “Enhancing the Functions of National Universities (for organizational development and projects), we started to establish the Global Station for Quantum Medical Science and Engineering (GSQ) in the Global Institution for Collaborative Research and Education (GI-CoRE), under the direct direction of the president of Hokkaido University. We brought outstanding faculty members from Hokkaido University and Stanford University together at the Hokkaido University campus in Sapporo, and worked to develop the GSQ further. At the same time, a global station was established at the Graduate School of Veterinary Medicine, resulting in the establishment of two smaller scale WPI at Hokkaido University.
Fig. 4: Briefing materials for the establishment of the GI-CoRE GSQ
For the six years from 2014 to 2019, research unit members of Stanford University at the GI-CoRE GSQ including Ruijiang Li stayed at Hokkaido University for half-year or one year periods. In the latter half of this period, Yi Cui and Yusuke Nomura, who had been employed as GSQ postdoctoral fellows by Hokkaido University, were employed as postdoctoral fellows by Stanford University in California. Also, Minami and Onodera of Hokkaido University, who went to Stanford University to participate in joint research, and Khin Khin Tha and Kenneth Sutherland, who conducted joint research on radiomiscs and artificial intelligence between Hokkaido University and Stanford University, were recognized by Stanford University as visiting scientists.
The most important mission of GI-CoRE GSQ is to organize summer schools for medical physics and radiation biology. Every year, we invite eminent professors from Stanford University to our campus in Sapporo and have them give lectures in English with us. We also contribute to the Summer Institute, which offers lectures for all graduate schools of Hokkaido University. From the start of this, we have held seven summer schools, with the help of faculty who were scheduled to be in charge of the Graduate School of Biomedical Science and Engineering, Umegaki and Yasui Hironobu of Hokkaido University, and Naruhiro Matsufuji and Yutaka Takahashi from other institutions. The summer school on medical physics was very popular and we had more than 100 applicants at its peak from all over the world for about 20 places. The summer school on radiation biology was also very popular, involving practical training in molecular biology, and the participants returned home very satisfied.
Fig. 5 The 4th GI-CoRE GSQ Summer School and the 7th GI-CoRE GSQ Symposium
7. Establishment of “Graduate School of Biomedical Science and Engineering”
There was another reason why the idea of “inviting a researcher unit” was approved to be included in a special budget project for the next academic year in 2013. At the time, graduate school students and faculty belonged to the same unit as the “Graduate School”. As an educational reform, the university was promoting the idea to separate “Research faculty” where faculty members belong from the “Graduate School” where graduate students belong”. However, no one was interested in the idea because many people thought that there was no obvious benefit to the Graduate School of Medicine or Graduate School of Dentistry to be separated into a Graduate School and a Research Faculty, and that it would increase the burden of education. Under these circumstances, the university head office requested us to present a plan that combined “inviting a researcher unit from an overseas institution” as described above and in the “organizational reform to separate Research Faculty from the Graduate School” to be able to realize international collaborative education.
These proposals for changes happened to occur at the same time as the Graduate School of Medicine secured support from the “Cancer Professional Training Program” of the Ministry of Education, Culture, Sports, Science and Technology (MEXT), and started a “Medical Physicist Program” for master’s and doctoral program students at the three graduate schools of medicine, engineering, and science, working with biomedical science and engineering researchers all present at Hokkaido University, and to be participating in the endowed chair of Molecular Tracking and Radiation Medicine of Hokkaido University Hospital and the FIRST project. In such a situation, those involved in the “Medical Physicist Program” were happy with that because the reorganization of the Graduate School of Medicine into a graduate school and a research faculty would eliminate the necessity for the three graduate schools each to conduct the program separately. Further, the university head office said that if we combine an “invited researcher unit from an overseas institution” in the project and the organizational reform to separate the research faculty from the graduate school, the university would permit employment of full-time faculty for those on time limited fixed terms (equivalent to 2.5 points) adding the President's Discretionary Funds to the special funds from MEXT. This proposal from the head office was a convenient change for those involved in the FIRST project, which employed many researchers with external funds.
Shirato and colleagues collected materials from the time of establishment of the Graduate School of Life Science and the Graduate School of Chemistry to learn about the structure of graduate schools and research faculty, and came up with the idea of establishing the Graduate School of Biomedical Engineering and Science separately from the Graduate School of Medicine. This would be feasible as Shirato realized that by assigning specially appointed faculty members from the Innovation projects, the FIRST, GI-CoRE programs, and visiting scientists from Stanford University as full-time faculty members of the “Graduate School of Biomedical Science and Engineering”, it would become possible to provide international collaborative education as expected by the head office without using any of the existing personnel dedicated funding of the Graduate School of Medicine. The prospective faculty members of the Graduate School of Biomedical Science and Engineering could also play active roles in undergraduate education, and as the staff involved are medical doctors and medical physicists involved in proton beam therapy and high-precision radiation therapy at Hokkaido University Hospital, this would benefit the medical education and hospital operation, and reduce the costs to the School of Medicine and University Hospital. For these reasons, Shirato explained to the parties concerned that there is an advantage in that faculty members of the graduate school of medicine will be able to contribute and take charge at other graduate schools. There also was an additional issue that would go away with this arrangement: the university head office had repeatedly pointed out, to the Dean of the Graduate School of Medicine, that with the rate of enrollment of the doctoral program of the Graduate School of Medicine remaining below 90% of the 100-student enrollment limit, that there was a risk of the number of faculty being reduced if the capacity could be satisfied by reducing the limit of graduate school enrollment. For this reason, if we transferred part of the graduate students of the Graduate School of Medicine to that of Biomedical Science and Engineering and made the rate of enrollment 100% by “the reorganization of the Graduate School of Medicine into a Graduate School of Medicine / Graduate School of Biomedical Science and Engineering / Faculty of Medicine, we would be able to improve the enrollment to 100%, and, the total number of faculty staff of the Graduate School of Medicine will increase by the number of faculty of the Graduate School of Biomedical Science and Engineering. The benefits for the Graduate School of Medicine were clear. Finally, on August 25, 2016 a Faculty Meeting of the Graduate School of Medicine approved the reorganization of the Graduate School of Medicine into the Graduate School of Medicine / Graduate School of Biomedical Science and Engineering / Faculty of Medicine. Since then, the rate of enrollment of the doctoral program of the Graduate School of Medicine has increased, and we have achieved our goal every year.
Fig. 6 Brochure of the Graduate School of Biomedical Science and Engineering at the establishment
In early 2013, there were only few full-time faculty who were able to take charge of courses at the Graduate School of Biomedical Science and Engineering. However, we gradually recruited specially appointed faculty who had been employed with external funds through special funds and the President's discretionary quota, and recommended them for full-time faculty positions in these departments. We also asked for the cooperation of Ryusuke Suzuki and Masaya Tamura, who were officially employed as medical physicists at the University Hospital, and Masayuki Aikawa of the Graduate School of Science, who played active roles in the establishment of the “Medical Physicist Program” at the “Cancer Professional Training Program” provided in the Graduate School of Science, and prepared the establishment of the Graduate School of Biomedical Science and Engineering. Finally, we asked for the help of researchers affiliated to the Graduate School of Medicine, the Graduate School of Dentistry, the Graduate School of Science, the Graduate School of Engineering, the Graduate School of Health Sciences, the University Hospital, and the Isotope Center, and were able to obtain the approval of the heads of their affiliated departments.
Through these processes the Graduate School of Biomedical Science and Engineering was officially established at Hokkaido University in 2017. We decided to assign two supervisors per student, one from the medical/biological field and the other from the physical/engineering field. The number of students for the master’s program (2-year) was 12, and that for the doctoral program (3-year) was 6. Every year we receive applications from students with a bachelor’s degree in science and engineering who wish to utilize their knowledge and skills in the development of medical devices or to work as medical physicists or dosimetrists in hospitals and these can now be better accommodated. To date about 30 students completed the programs and are active in society. The job placement rate for applicants is almost 100% every year. Many of these graduates are active in major companies, but some choose careers as researchers in “Biomedical Science and Engineering” in the doctoral program. The number of graduated students who obtained their doctoral degrees while working in companies has increased.
8. “Integrating” Educational Organization for Biomedical Science and Engineering Research
From 2019, we have received high acclaim for the achievements and future potential of research in biomedical science and engineering and human resource training at the Graduate School of Biomedical Science and Engineering. The Ministry of Education, Culture, Sports, Science and Technology (MEXT) has approved the integration of the budget (a change from a time-limited budget in management expense grants to a general budget item among the operating grants) for personnel and research expenses to full-time faculty at the Graduate School of Biomedical Science and Engineering.
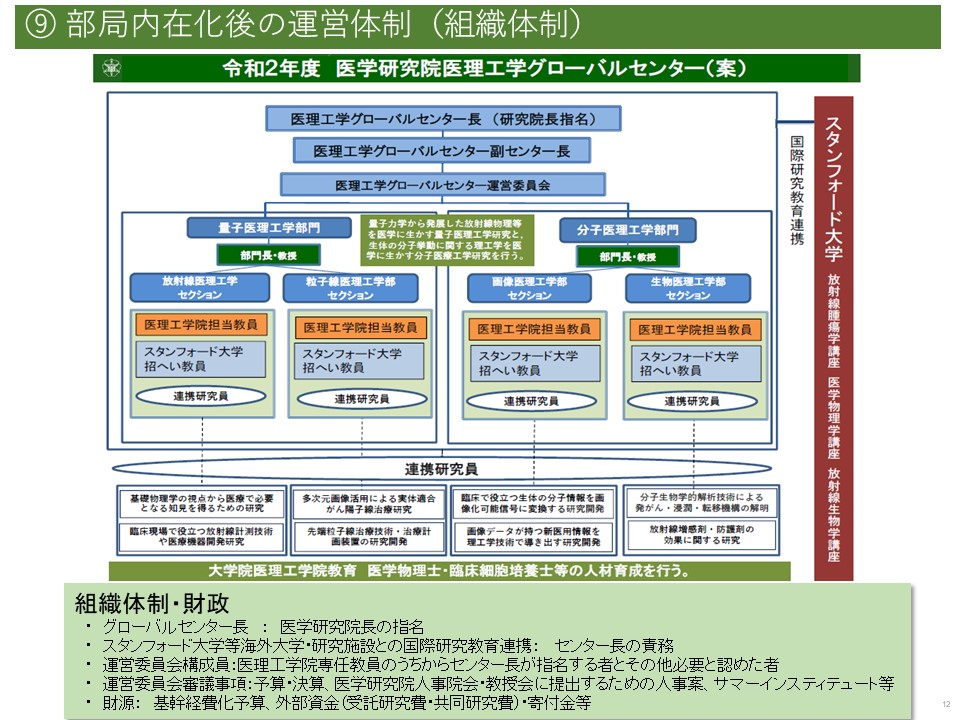
Fig. 7 Materials used in the Presidential hearing for integrationFig. 8 Organizational chart of the GCB at the time of establishment used in the Presidential hearing
The university head office proposed that for personnel expenses, we may use 100% of the funds, but if for research, the allocation for the Graduate School of Biomedical Science and Engineering is 25%, and the remaining 75% is for the university head office to allocate. Since this would result in inefficient use of the funds for research, we considered that a rational option would be to integrate (combine) most of the funds as personnel expenses for “non-fixed term positions in the Graduate School of Biomedical Science and Engineering” to allow the employed medical doctors and medical physicists to be able to contribute to the hospital management. It was decided that this budget item was included in the planned budget with a lump sum of “8.2 personnel cost points” assigned to the Faculty of Medicine, which would be responsible for organizing the entire project, and that the Faculty of Medicine would consult with the relevant departments about the use. The Faculty of Medicine provided detailed materials to the Future Planning Committee in October 2019 and to the Faculty Council in November 2019 for their discussions and this option was approved.
In the Faculty of Medicine, three regular employment positions (one professor, one associate professor, and one assistant professor) were assigned to the Department of Radiological Science and Engineering, creating a basic department equivalent to other departments managed by the Graduate School of Medicine. Shinichi Shimizu, Takayuki Hashimoto, and Kentaro Nishioka were appointed as the first professor, associate professor, and assistant professor, respectively.
The funds (1.0 points) for professor in the Department of Proton Beam Therapy and Medicine, Center for Collaborative Research, Faculty of Medicine will be assigned to the entire Faculty of Medicine after the 2022 academic year, when Hiroki Shirato retires, to clearly establish that this is a positive measure for the Faculty of Medicine.
As a successor organization to the integrated GI-CoRE GSQ, the Global Center for Biomedical Science and Engineering (GCB) will be established within the Faculty of Medicine, with one professor or associate professor, one associate professor, and one assistant professor in the Graduate School of Biomedical Science and Engineering. In the first year, these posts were assigned to the following staff: Khin Khin Tha (associate professor), Jin-Min NAM (lecturer), and Kenneth Sutherland (assistant professor).
For the other departments, provided that the following staff will be in charge of the Graduate School of Biomedical Science and Engineering, one professor of the Faculty of Science was assigned to the field of basic medical physics of the Graduate School of Biomedical Science and Engineering, and one associate professor of the Faculty of Engineering was assigned to the field of radiological physics. Further, two professors or associate professors at the Faculty of Health Sciences were in charge of the medical physics field and the medical image analysis field. The director of the Faculty of Medicine and directors of other faculties involved signed a memorandum to assign (for a non-fixed term) one assistant professor to reduce the educational burden of the two professors or associate professors at the Faculty of Health Sciences of the director and one clerical staff of the Graduate School of Biomedical Science and Engineering.
From the Faculty of Engineering, Taeko Matsuura filled the post, followed by Naoki Miyamoto, and Seishin Takao.
From the Faculty of Science, we welcomed Masayuki Aikawa, who had been working under the President’s discretionary quota, to belong to the regular faculty utilizing the integrated personnel funds from 2021.
From the Faculty of Health Sciences, Chietsugu Kato and Masayori Ishikawa were in charge of the Graduate School of Biomedical Science and Engineering, and an assistant professor was hired.
In addition, the Graduate School of Dentistry was reorganized into the Graduate School of Dentistry and the Faculty of Dentistry. Fumihiro Higashino was in charge of the Graduate School of Biomedical Science and Engineering. Under Professor Yuji Kuge, who changed the major association from the Graduate School of Medicine to the Graduate School of Biomedical Science and Engineering, Hironobu Yasui and Yuki Mizuno were officially welcomed as full time, tenured staff.
Many of these people have been active in biomedical science and engineering research and development at Hokkaido University for many years as specially appointed faculty with limited terms of office. If their tasks were only research and development, the they would have had to leave Hokkaido University as soon as the research funding expired, and the research itself would then often be forgotten. The establishment of the Graduate School of Biomedical Science and Engineering was an important step in the development of the available specialized staff in Biomedical Science and Engineering, with the understanding of MEXT, people at Hokkaido University Head Office, and the Faculty of Medicine. Currently, medical physics researchers, radiation biologists, and machine learning researchers are training researchers in the “biomedical science and engineering” field at the Graduate School of Biomedical Science and Engineering. Again, quiet “backroom effort” had been the key to maintaining research useful in the world to be able to progress in a timely fashion. We expect that the full-time faculty members of our graduate school will engage in further backroom work to develop “biomedical science and engineering” by utilizing the “integrated” faculty positions described above.
9. Global Center for Biomedical Science and Engineering
From 2019, together with the “integration” of the research and educational organizations for biomedical science and engineering into the Graduate School of Biomedical Science and Engineering, we established the Global Center for Biomedical Science and Engineering (GCB). The purpose of the GCB is to maintain the system that has been developed as the GI-CoRE GSQ Stanford University Unit, to maintain courses that allow students to graduate exclusively in English at the Graduate School of Biomedical Science and Engineering, and to provide international collaborative education in biomedical science and engineering at the annual Summer Institute. One professor or associate professor, one associate professor, and one assistant professor of the GCB are called for in continuing and developing international collaborative research in the GCB with other full-time faculty of the Graduate School of Biomedical Science and Engineering.
In addition, as administrative staff for the GCB like in its predecessor the GSQ, one specific professional and two administrative assistants who were fluent in English were budgeted for, in addition to the researchers.
In the GI-CoRE GSQ there were two units, the Hokkaido University Unit and the Stanford University Unit, but in the GCB these were reorganized into organizations corresponding to the fields of biomedical science and engineering. More specifically, the Center is comprised of two sections, the Quantum Biomedical Science and Engineering Section and the Molecular Biomedical Science and Engineering Section. The former has a Radiation Medical Science and Engineering Section and a Particle Medical Science and Engineering Section, and the latter has an Imaging Medical Science and Engineering Section and a Biomedical Science and Engineering Section. In each section, a mix of faculty from the Hokkaido University Unit and the Stanford University Unit was assigned to the respective duties.
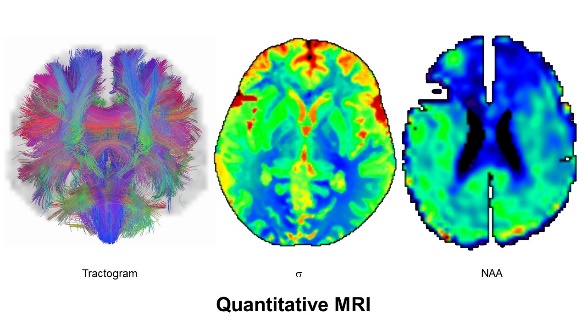
Fig. 9 The GCB MRI medical imaging research and molecular imaging research at the GCB
It was decided that the GCB will continue to use and manage the wet lab benches built during the GI-CoRE GSQ years, the animal experiment equipment purchased with special funds, and the workstations used for simulation research.
Although the research budget of the GCB available for use at our discretion is limited because much of the budget is allocated to personnel expenses, it is possible to subsidize the travel and accommodation expenses of graduate students and researchers from overseas, and to invite lecturers from outside Japan to travel here by economy class for the summer institute and summer school.
The establishment of the GCB provides a basis for talented researchers in biomedical science and engineering and for non-Japanese researchers, who have had unstable work conditions after being employed with large external funds when they were starting out as researchers. At the GCB they are able to conduct research as regular employees of Hokkaido University without worrying too much about tenure. We believe this is a big step forward in the history of biomedical science and engineering in Japan, although the scale is still small.
Large-scale research and development projects with a predetermined term supported by large, eye-catching external funds are not always an opportunity where you engage in biomedical science and engineering research. The GCB will be able to provide the time for individual researchers to more calmly and unhurriedly assess their vision of the future, start with a small study, and bring about essential and remarkable changes based on that study. In the future, the members of the GCB will change, but we have great expectations that research that will win Nobel Prizes and attract venture companies that will develop globally will be developed at the GCB.
10. Medical Physics Department in the Hospital
As detailed above, and since the 1980s, many medical physicists who are employed as faculty with doctoral degrees and dosimetrists with master's degrees in science and engineering having an accurate and comprehensive understanding of radiation science and engineering have been working in university hospitals in Europe and the U.S. There smaller facilities usually employ several medical physicists and dosimetrists, and there are dozens of these specialized professionals at larger facilities. However, in Japan such professionals working in university hospitals were rare, and until the early 2000s, there were at most one or at times no medical physicists and dosimetrists at both Hokkaido University Hospital and the National Cancer Center in Tsukiji in Tokyo.
To respond to this situation, Hokkaido University established the endowed chair of Molecular Tracking and Radiation Medicine in the University Hospital, and worked on the training of medical physicists through the “Human Resource Development Plan for Cancer”. Further, we held radiotherapy quality control committee meetings led by Ryusuke Suzuki on a regular basis, and built a quality control framework for intensity modulated radiation therapy (IMRT). Following this, it became possible to employ medical physicists with external funds such as with NEDO and AMED, and as the demands for treatment planning for IMRT in hospitals sharply increased, medical physicists and researchers aiming to become medical physicists have dealt with treatment planning for IMRT, as practical training. Further, after the start of proton beam therapy using FIRST, the university hospital came to evaluate the contribution of medical physicists highly in the hospital management, and four medical physicists were officially hired as assistant professors based on a detailed income and expenditure plan. In addition, two medical radiologists were officially hired as dosimetrists and two as proton irradiologist.
In 2019 the Department of Medical Physics was officially established in the University Hospital. The Department of Medical Physics is also involved in the education of graduate students in collaboration with Kikuo Umegaki, Taeko Matsuura, Naoki Miyamoto, and others who were faculty of the Department of Engineering at the Faculty of Engineering, who also contributed greatly to the establishment of the Graduate School of Biomedical Science and Engineering. There, a course for biomedical physicists is offered, and practical training in the Department of Medical Physics in the hospital is included in the curriculum of the doctoral program.
For the future, we hope that the career path for medical physicists will become clearer by making it a nationally approved qualification. To make this possible, it is important to have educational programs in Japan that are different from those of radiology technologists, clinical laboratory technologists, or clinical engineering technologists. If universities have graduate schools of biomedical science and engineering, and university hospitals establish medical physics departments as an employment option for graduates of biomedical science and engineering schools, necessary like a car needs to have wheels on both sides, this will be a model for other universities as a basis for human expertise development, and would be a significant step towards creating a national qualification for medical physicists.
11. Conclusion
It has been only 200 years since the atomic and molecular theories of Dalton and Avogadro, 100 years since the quantum mechanics of Heisenberg and Schrodinger, and 70 years since Schrodinger’s “What is Life?” Looking back on the long history of medicine, and considering the complexity and difficulty of modern quantum science and engineering, I think it highly probable that graduates of the Graduate School of Biomedical Engineering will invent and develop medical technologies and devices that are unimagined today.
Considering the future of medicine, something which cannot be handled by medical doctors alone, I believe that the significance of the Global Center for Biomedical Science and Engineering, Faculty of Medicine, will grow and become more central in the future.
I sincerely hope and wish for you to provide us with continued advice, cooperation, and encouragement (Hiroki Shirato, March, 2021).
Tsujii H, Kamada T, Matsuoka Y, Takamura A, Akazawa T, Irie G. The value of treatment planning using CT and an immobilizing shell in radiotherapy for paranasal sinus carcinomas. Int J Radiat Oncol Biol Phys. 1989 Jan;16(1):243-9. doi: 10.1016/0360-3016(89)90037-0. PMID: 2912946.
Shirato H, Suzuki K, Nishioka T, Kamada T, Kagei K, Kitahara T, Morisawa H, Tsujii H. Precise positioning of intracranial small tumors to the linear accelerator's isocenter, using a stereotactic radiotherapy computed tomography system (SRT-CT). Radiother Oncol. 1994 Aug;32(2):180-3. doi: 10.1016/0167-8140(94)90105-8. PMID: 7972912.
Aoyama H, Shirato H, Tago M, Nakagawa K, Toyoda T, Hatano K, Kenjyo M, Oya N, Hirota S, Shioura H, Kunieda E, Inomata T, Hayakawa K, Katoh N, Kobashi G. Stereotactic radiosurgery plus whole-brain radiation therapy vs stereotactic radiosurgery alone for treatment of brain metastases: a randomized controlled trial. JAMA. 2006 Jun 7;295(21):2483-91.
Shimizu S, Shirato H, Kagei K, Nishioka T, Bo X, Dosaka-Akita H, Hashimoto S, Aoyama H, Tsuchiya K, Miyasaka K. Impact of respiratory movement on the computed tomographic images of small lung tumors in three-dimensional (3D) radiotherapy. Int J Radiat Oncol Biol Phys. 2000 Mar 15;46(5):1127-33. doi: 10.1016/s0360-3016(99)00352-1. PMID: 10725622.
Seppenwoolde Y, Shirato H, Kitamura K, Shimizu S, van Herk M, Lebesque JV, Miyasaka K. Precise and real-time measurement of 3D tumor motion in lung due to breathing and heartbeat, measured during radiotherapy. Int J Radiat Oncol Biol Phys. 2002 Jul 15;53(4):822-34. doi: 10.1016/s0360-3016(02)02803-1. PMID: 12095547.
Berbeco RI, Nishioka S, Shirato H, Chen GT, Jiang SB. Residual motion of lung tumours in gated radiotherapy with external respiratory surrogates. Phys Med Biol. 2005 Aug 21;50(16):3655-67. doi: 10.1088/0031-9155/50/16/001. Epub 2005 Jul 28. PMID: 16077219.
Takao S, Miyamoto N, Matsuura T, Onimaru R, Katoh N, Inoue T, Sutherland KL, Suzuki R, Shirato H, Shimizu S. Intrafractional Baseline Shift or Drift of Lung Tumor Motion During Gated Radiation Therapy With a Real-Time Tumor-Tracking System. Int J Radiat Oncol Biol Phys. 2016 Jan 1;94(1):172-180. doi: 10.1016/j.ijrobp.2015.09.024. Epub 2015 Sep 25. PMID: 26700711
Matsuura T, Miyamoto N, Shimizu S, Fujii Y, Umezawa M, Takao S, Nihongi H, Toramatsu C, Sutherland K, Suzuki R, Ishikawa M, Kinoshita R, Maeda K, Umegaki K, Shirato H. Integration of a real-time tumor monitoring system into gated proton spot-scanning beam therapy: an initial phantom study using patient tumor trajectory data. Med Phys. 2013 Jul;40(7):071729. doi: 10.1118/1.4810966. PMID: 23822433.
Shimizu S, Miyamoto N, Matsuura T, Fujii Y, Umezawa M, Umegaki K, Hiramoto K, Shirato H. A proton beam therapy system dedicated to spot-scanning increases accuracy with moving tumors by real-time imaging and gating and reduces equipment size. PLoS One. 2014 Apr 18;9(4):e94971. doi:10.1371/journal.pone.0094971. PMID: 24747601; PMCID: PMC3991640.
Yamada T, Miyamoto N, Matsuura T, Takao S, Fujii Y, Matsuzaki Y, Koyano H, Umezawa M, Nihongi H, Shimizu S, Shirato H, Umegaki K. Optimization and evaluation of multiple gating beam delivery in a synchrotron-based proton beam scanning system using a real-time imaging technique. Phys Med. 2016 Jul;32(7):932-7. doi: 10.1016/j.ejmp.2016.06.002. Epub 2016 Jun 10. PMID:27296793.
Shimizu S, Matsuura T, Umezawa M, Hiramoto K, Miyamoto N, Umegaki K, Shirato H. Preliminary analysis for integration of spot-scanning proton beam therapy and real-time imaging and gating. Phys Med. 2014 Jul;30(5):555-8
EC TR 62926:2019. Medical electrical system – Guidelines for safe integration and operation of adaptive external-beam radiotherapy systems for real-time adaptive radiotherapy. https://webstore.iec.ch/publication/34482
Hashimoto T, Shimizu S, Takao S, Terasaka S, Iguchi A, Kobayashi H, Mori T, Yoshimura T, Matsuo Y, Tamura M, Matsuura T, Ito YM, Onimaru R, Shirato H. Clinical experience of craniospinal intensity-modulated spot-scanning proton therapy using large fields for central nervous system medulloblastomas and germ cell tumors in children, adolescents, and young adults. J Radiat Res. 2019 Jul 1;60(4):527-537.
Nishioka K, Prayongrat A, Ono K, Onodera S, Hashimoto T, Katoh N, Inoue T, Kinoshita R, Yasuda K, Mori T, Onimaru R, Shirato H, Shimizu S. Prospective study to evaluate the safety of the world-first spot-scanning dedicated, small 360-degree gantry, synchrotron-based proton beam therapy system. J Radiat Res. 2018 Mar 1;59(suppl_1):i63-i71.